1. Introduction
Midazolam (MDZ), 1-benzodiazepine, is widely used to sedate patients in intensive care units and to induce anesthesia because of the rapid onset and short duration of its effects (Nordt and Clark,
1997). MDZ is rapidly and extensively metabolized by the liver and intestinal microsomal enzymes (Heizmann and Ziegler,
1981; Kronbach et al.,
1989). Many factors, such as age and sex (Hunt et al.,
1992; Gibbs and Hosea,
2003; Wojnowski,
2004; Cotreau et al.,
2005), concomitant medication (von Moltke et al.,
1996), and hepatic function (Gibbs and Hosea,
2003), may influence the activity of CYP3A isoforms.
The bispectral index (BIS) is a processed electroencephalographic parameter that has been reported to correlate well with hypnotic depth during anesthesia (Glass et al.,
1997; Rosow and Manberg,
2001). Therefore, BIS is widely used to quantify the hypnotic effects of anesthetics and can serve as a tool to monitor and titrate the pharmacodynamic effects of anesthetic drugs (Sandin et al.,
2008). Dahaba et al. (
2008) graded encephalopathy using the West Haven criteria in a multicenter study, and demonstrated that the BIS can be used to grade the degree of hepatic encephalopathy in patients with chronic liver disease. They also found that BIS displayed a weak to moderate correlation with the serum concentration of ammonia and the Child-Pugh score. In patients with obstructive jaundice, Yang et al. (
2010) found an increased sensitivity to isoflurane and a prolonged recovery time compared with controls.
Previous studies have shown that both the pharmacokinetics (MacGilchrist et al.,
1986; Pentikäinen et al.,
1989) and pharmacodynamics (MacGilchrist et al.,
1986) of MDZ were significantly impaired in patients with hepatic cirrhosis. The effects of liver function on sensitivity to MDZ and prediction of the BIS for loss of consciousness (LOC) remain unclear. The main focus of this research was to examine the influence of liver function on the MDZ concentration and the BIS value at the time of LOC in patients. Our hypothesis was that liver function would influence the concentration of MDZ (EC
50) and the BIS value (BIS
50) at which 50% of patients lose consciousness. The results may provide guidance for clinicians using MDZ and the BIS when treating patients with liver malfunction.
2. Materials and methods
2.1. Subjects
Between June 2009 and May 2011, 45 patients were studied. Thirty of these patients diagnosed with cholelithiasis were scheduled for laparoscopic cholecystectomy, including 15 patients with normal liver function (normal group), and 15 with moderately abnormal liver function based on ultrasonic diagnosis of a moderately fatty liver and elevated alanine transaminase levels of less than three times normal (moderate group). The other 15 patients with end-stage liver disease (severe group) underwent liver transplantation. The protocol (reference number 20090150) was approved on 15 May 2009 by the Ethics Committee of the First Affiliated Hospital, School of Medicine, Zhejiang University (Hangzhou, China). Each patient gave his/her informed consent to participate. Patients were excluded from the study if they had serious impairment of respiratory, cardiovascular, renal, or endocrine function, or if they had received medication likely to interfere with the study’s results.
2.2. Procedure
No patients received premedication. After each patient arrived in the operating theatre, a radial artery was canulated for taking blood samples and continuous measurements of invasive blood pressure. Two intravenous trocars were placed in large forearm veins, one for infusion of MDZ and the other for infusion of fluid. The electrocardiogram (ECG), heart rate (HR), end-tidal carbon dioxide partial pressure (EtCO
2), oxyhemoglobin saturation (SpO
2), and invasive arterial blood pressure (ABP) were monitored throughout the study using a multifunction monitor (Datex-Ohmeda, Hoevelaken, the Netherlands). The depth of sedation of patients was assessed using a BIS sensor and the BIS index was recorded digitally on a BIS monitor, Model A-2000TM (Aspect Medical System, Natick, MA, USA).
2.3. Drug administration and blood sample analysis
Before the administration of MDZ, all patients received crystalloid solution (acetated Ringer’s solution) at 20 ml/kg body weight. With patients breathing 100% oxygen (4 L/h) through an oxygen mask, MDZ was administered by a target-controlled infusion (TCI) using a TCI pump (Graseby 3500 pump, Graseby Medical Ltd., Colonial Way, Watford, Herts, UK) containing the pharmacokinetic model of Greenblatt et al. (
1984): elimination rate constant (
k
10), 0.015 min
−1; central compartment to peripheral compartment transfer rate constant (
k
12), 0.0139 min
−1; peripheral compartment to central compartment transfer rate constant (
k
21), 0.135 min
−1; plasma-effect compartment balance rate constant (
k
e0), 0.124 min
−1. The system can display the total dose of MDZ at any time after infusion of MDZ is discontinued.
The MDZ infusion started from the target concentration of 50 ng/ml, which was increased by increments of 50 ng/ml every 30 s until LOC occurred, then the target concentration was set to zero to discontinue the infusion. Patients were checked every 5 s and LOC was determined by the loss of response to a verbal command, as described by Milne et al. (
2003). When a patient suffered dyspnea, appropriate respiratory support was supplied. Hypotension was defined as a reduction of systolic blood pressure by more than 30% of the pre-anesthetic value or a systolic blood pressure of less than 90 mmHg. Patients with hypotension received treatment with 6 mg of intravenous ephedrine and 300 ml of crystalloid fluids. Bradycardia was defined as an HR of less than 55 beats/min and was treated by administering 0.5 mg of intravenous atropine. On completion of the experimental evaluation, anesthesia started.
An arterial blood sample (5 ml) for measurement of the concentration of MDZ was drawn from the indwelling radial cannula at two time points: before and at the time of LOC. All samples were collected in heparinized tubes and centrifuged within 30 min of collection. The plasma was transferred to polypropylene tubes and frozen at −20 °C until assayed. MDZ concentrations in plasma were measured within 14 weeks by high-performance liquid chromatography (HPLC) with fluorescence detection (Luo et al.,
2006).
2.4. Statistical analysis
The following computer packages were used: Excel 2007 (Microsoft, Redmond, WA, USA), SPSS 11.5 (SPSS Inc., Chicago, IL, USA), and G*Power 3.0.10 (University Kiel, Germany). Sample size estimation was based on a type I statistical error of 0.05 and a type II statistical error of 0.2 to detect a 20% reduction in the measured plasma concentration of MDZ required for LOC. It was estimated that 15 patients would be necessary for each of the three groups. Demographic data are presented as a mean±standard deviation (SD) or count (number) as appropriate. Averages were analyzed using analysis of variance (ANOVA; more than two groups), while counts or proportions were analyzed using Fisher’s exact test. The EC
50 of MDZ and BIS
50 for LOC were estimated by probit analysis. Statistical significance was defined as
P<0.05 (two-tailed). Correlations between parameters were evaluated by simple and multiple linear regression analysis. Assessment of the linear association between the probability of unconsciousness and the measured MDZ concentration and corresponding BIS at the time of LOC was performed using logistical regression. The curves were fitted using Pearson goodness-of-fit tests with a natural response rate calculated from the data.
3. Results
Twenty-two men and twenty-three women were recruited in our study. Demographic data for all the subjects are presented in Table
1. There were no significant differences in age, body weight, or height among the three groups. Compared with the normal group, the levels of alanine transaminase (ALT) in the moderate and severe groups were significantly higher (
P<0.01), while compared with the severe group, the serum albumin (ALB) levels were significantly higher in normal and moderate groups (
P<0.01). The ABP, HR, and SpO
2 in all patients remained within normal limits throughout the study. The number of patients suffering from hypotension did not differ among the groups. Two patients received 6 mg ephedrine boluses during the study because of hypotension.
Table 1
Characteristics and hepatic function of the subjects
| Group |
Age (year) |
Weight (kg) |
Height (m) |
Male/female |
ALT (U) |
ALB (g/ml) |
| Normal (n=15) |
39±9 |
61±8 |
1.66±0.08 |
7/8 |
25±5b
c
|
41±3c
|
| Moderate (n=15) |
42±11 |
62±10 |
1.68±0.09 |
8/7 |
110±9c
|
40±2c
|
| Severe (n=15) |
43±11 |
64±7 |
1.67±0.08 |
7/8 |
508±173 |
23±3 |
Data are reported as mean±SD, except for the values of male/female
b
P<0.01, vs. the moderate group
c
P<0.01, vs. the severe group
ALT: alanine transaminase; ALB: albumin
The linear range of MDZ detected was 20–500 ng/ml and the limit of detection of MDZ in plasma was about 15 ng/ml. The coefficient of variation of this HPLC method was less than 10% within the range of concentrations measured in this study. The results for the EC
50 of MDZ and the BIS
50 for LOC (95% confidence interval (CI)) for each group are listed in Table
2. Logistic regression analysis showed that the EC
50 of MDZ for LOC in the severe group was significantly lower (
P<0.05), while the BIS
50 was significantly higher compared with the corresponding values in the normal and moderate groups (
P<0.05). Regression analysis showed a coefficient of correlation between the concentration of MDZ at LOC and ALT (
r=−0.542), and a correlation with ALB (
r=0.590). The coefficient of correlation between the BIS at LOC and ALT was
r=0.630, and
r=0.681 for the correlation with ALB. All correlation coefficients from the regression analysis were much lower than 0.5, indicating that ALT and ALB explained less than 50% of the concentration of MDZ and of the BIS at LOC.
Table 2
Results of EC50 of midazolam (MDZ) and BIS50 for loss of consciousness (LOC)
| Group |
EC50 (ng/ml) |
BIS50
|
| Normal (n=15) |
310.4 (226.5–317.7)*
|
51 (49–61)*
|
| Moderate (n=15) |
294.8 (246.0–316.3)*
|
52 (48–59)*
|
| Severe (n=15) |
220.0 (188.3–233.2) |
69 (67–72) |
Values in parentheses are 95% confidence intervals (CIs)
*
P<0.05 vs. the severe group
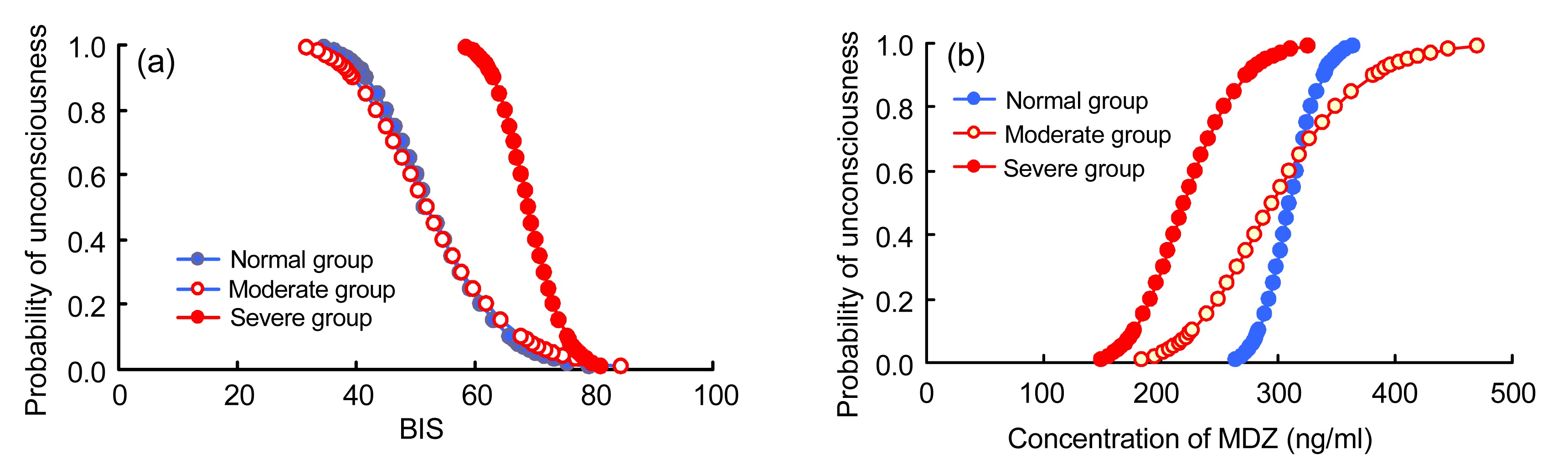
Fig.
1 demonstrates the relationship between the probability of unconsciousness and the concentration of MDZ and the BIS. Compared with the normal and moderate groups, in the severe group the MDZ concentration curve shifted to the left, whereas the BIS curve shifted to the right.
Fig.1
Probability of unconsciousness versus the BIS values (a) and midazolam (MDZ) concentration (b)
Compared with the normal and moderate groups, in the severe group the MDZ concentration curve shifted to the left, whereas the BIS curve shifted to the right
The estimates of the logistic model for plasma MDZ concentration and the BIS value at LOC are shown in Table
3. None of the goodness-of-fit Chi square values were significant, and so no heterogeneity factor was used in the calculation of confidence limits.
Table 3
Estimates of the probit models for the plasma concentration of midazolam (MDZ) and the BIS value at loss of consciousness (LOC)
| Group |
Independent variable |
Estimate of natural response rate |
Intercept*
|
Regression coefficient *
|
P-value for Pearson goodness-of-fit |
| Normal (n=15) |
MDZ concentration |
0.26 |
−82.91±38.50 |
33.27±15.36 |
0.660 |
| BIS |
0.05 |
22.28±5.28 |
−12.95±3.17 |
1.000 |
| Moderate (n=15) |
MDZ concentration |
0.17 |
−28.24±7.77 |
11.44±3.07 |
0.921 |
| BIS |
0 |
18.79±3.59 |
−10.96±2.17 |
0.999 |
| Severe (n=15) |
MDZ concentration |
0.15 |
−32.14±9.53 |
13.71±3.99 |
0.842 |
| BIS |
0.08 |
60.42±12.77 |
−32.86±7.01 |
1.000 |
*Data are reported as mean±standard error (SE)
4. Discussion
To the best of our knowledge, this is the first study to specifically assess the effect of hepatic function on the EC
50 of MDZ and the BIS
50 at LOC. The main purpose of the study was to explore whether hepatic function influences the sensitivity to MDZ. The results indicated that patients with severe hepatic dysfunction required less MDZ to lose consciousness. The study also showed that the patients with end-stage liver disease lost consciousness at higher BIS values than those with normal or moderately abnormal liver function.
Previous studies have reported conflicting findings concerning altered cerebral sensitivity to MDZ or other hipnotic drugs in cirrhotic patients. MacGilchrist et al. (
1986) showed that alcoholic cirrhosis was associated with significantly delayed elimination of MDZ and greater sedation after intravenous administration of MDZ. In a later study, Pentikäinen et al. (
1989) reported that the elimination of MDZ was significantly retarded, but not the hypnotic effects, in patients with cirrhosis. Yang et al. (
2010) reported that patients with jaundice needed a lower minimum alveolar concentration (MAC) of isoflurane than normal patients to achieve the same depth of anesthesia. On the contrary, being at the BIS-guided equal-anesthetic level, they have more hypotension and bradycardia during surgery than patients without hyperbilirubinemia. Song et al. (
2005) showed that the MAC for achieving a 50% probability of no response to a verbal command of desflurane for patients with obstructive jaundice decreased significantly compared with that for non-jaundiced controls (
P<0.001). Conflicting findings have been reported by Song et al. (
2009) concerning the influence of jaundice on sensitivity to propofol. Song et al. (
2009) demonstrated that obstructive jaundice with serum total bilirubin levels of from 7.8 to 362.8 μmol/L has no effect on propofol pharmacodynamics assessed by the BIS and mean arterial pressure. Wu et al. (
2013) demonstrated that patients with liver dysfunction required less propofol to attain an equal anesthetic level guided by the BIS. Our results are consistent with those from the pharmacodynamic study of volatile anesthetics by Yang et al. (
2010), and the studies by MacGilchrist et al. (
1986) and Wu et al. (
2013). Different results might arise partly from differences in study protocols.
The concept of the MAC for inhalation anesthetics is well known and widely used to ensure that patients receive adequate anesthesia, thus preventing intraoperative awareness (Zbinden et al.,
1994). A similar concept is applied to intravenous anesthetic agents and is known as the median effective concentration, the EC
50 (Smith et al.,
1994). This is a very practical clinical concept because it tends to predict the concentrations of propofol both in the plasma and in the effect site simulated by different pharmacokinetic models (White and Kenny,
1990; Shafer and Gregg,
1992; Smith et al.,
1994). Both the MAC for volatile anesthetics and median effect site concentrations for intravenous anesthetics can be expressed by a variety of clinical end-points such as tracheal intubation, extubation, body movement, awareness, recall, or hemodynamic responses. In the current study, we focused mainly on LOC.
Foley et al. (
1950) first reported that the delta activity of the visual electroencephalogram (EEG) correlated well with the conscious state of patients with hepatic coma. Dahaba et al. (
2008) revealed a complete separation between controls and each of the West Haven grades 1 to 4 based on the BIS, with BIS cut-off values of 95 for controls versus West Haven grade 1, 85 for grade 1 versus grade 2, 70 for grade 2 versus grade 3, and 55 for grade 3 versus grade 4, yielding agreement between the BIS classification and West Haven grades in 40 of 46 validation patients (87%). Thus, they concluded that the BIS represents a simple and objective neurophysiological measure for grading and monitoring the degree of involvement of the central nervous system in patients with chronic liver disease.
The results of the present study suggest that patients with hepatic encephalopathy are more sensitive to hypnotic drugs. A disorder between excitatory and inhibitory synaptic transmission in the parahippocampal gyrus might provide a possible explanation (Jenkins et al.,
1996; Franks and Lieb,
1998; Mennerick et al.,
1998; Yamakura and Harris,
2000). Further experiments are needed to explore the specific mechanism. In this study, some of the patients with end-stage liver disease were suffering different degrees of hepatic encephalopathy. Failure to recruit patients according to their degree of illness is one limitation of the present study. Further studies are needed to explore the possible influence of hepatic encephalopathy on the BIS
50 and EC
50 of hypnotics.
In summary, we have investigated the effect of hepatic function on the LOC and the BIS in patients. We demonstrated that patients with end-stage liver disease were more sensitive to MDZ and the prediction of the timing of LOC following MDZ treatment was affected, while there were no changes in patients with moderately abnormal hepatic function. Clinicians should be aware of the possible need to reduce anesthesia or the sedation dose of MDZ for patients with hepatic dysfunction.
Acknowledgements
We thank Dr. Fang-ping BAO, the anesthesiologist of the First Affiliated Hospital, School of Medicine, Zhejiang University, China, for his assistance during the experiments.
* Project supported by the Qianjiang Talents Project of the Technology Office in Zhejiang Province (No. 2012R10033) and the Clinical Scientific Research Funds of Zhejiang Provincial Medical Association (No. 2012ZYC-A72), ChinaCompliance with ethics guidelines Yu-hong LI, Rui HE, and Jin-guang RUAN declare that they have no conflict of interest.References
[1] Cotreau, M.M., von Moltke, L.L., Greenblatt, D.J., 2005. The influence of age and sex on the clearance of cytochrome P450 3A substrates.
Clin Pharmacokinet, 44(1):33-60.


[2] Dahaba, A.A., Worm, H.C., Zhu, S.M., 2008. Sensitivity and specificity of bispectral index for classification of overt hepatic encephalopathy: a multicentre, observer blinded, validation study.
Gut, 57(1):77-83.
[3] Foley, J.M., Watson, C.W., Adams, R.D., 1950. Significance of the electroencephalographic changes in hepatic coma.
Trans Am Neurol Assoc, 51:161-165.
[4] Franks, N.P., Lieb, W.R., 1998. Which molecular targets are most relevant to general anaesthesia?.
Toxicol Lett, 100-101:1-8.
[5] Gibbs, M.A., Hosea, N.A., 2003. Factors affecting the clinical development of cytochrome P450 3A substrates.
Clin Pharmacokinet, 42(11):969-984.
[6] Glass, P.S., Bloom, M., Kearse, L., 1997. Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane, and alfentanil in healthy volunteers.
Anesthesiology, 86(4):836-847.
[7] Greenblatt, D.J., Abernethy, D.R., Locniskar, A., 1984. Effect of age, gender, and obesity on midazolam kinetics.
Anesthesiology, 61(1):27-35.
[8] Heizmann, P., Ziegler, W.H., 1981. Excretion and metabolism of 14C-midazolam in humans following oral dosing.
Arzneimittelforschung, 31(12a):2220-2223.
[9] Hunt, C.M., Westerkam, W.R., Stave, G.M., 1992. Effect of age and gender on the activity of human hepatic CYP3A.
Biochem Pharmacol, 44(2):275-283.
[10] Jenkins, A., Franks, N.P., Lieb, W.R., 1996. Actions of general anaesthetics on 5-HT
3 receptors in N1E-115 neuroblastoma cells.
Br J Pharmacol, 117(7):1507-1515.
[11] Kronbach, T., Mathys, D., Umeno, M., 1989. Oxidation of midazolam and triazolam by human liver cytochrome P450IIIA4.
Mol Pharmacol, 36(1):89-96.
[12] Luo, N.F., Zhang, W.S., Jia, M.X., 2006. Determination of midazolam in plasma by RP-HPLC.
West China Pharm J, (in Chinese),21(4):384-385.
[13] MacGilchrist, A.J., Birnie, G.G., Cook, A., 1986. Pharmacokinetics and pharmacodynamics of intravenous midazolam in patients with severe alcoholic cirrhosis.
Gut, 27(2):190-195.
[14] Mennerick, S., Jevtovic-Todorovic, V., Todorovic, S.M., 1998. Effects of nitrous oxide on excitatory and inhibitory synaptic transmission in hippocampal cultures.
J Neurosci, 18(23):9716-9726.
[15] Milne, S.E., Troy, A., Irwin, M.G., 2003. Relationship between bispectral index, auditory evoked potential index and effect-site EC
50 for propofol at two clinical end-points.
Br J Anaesth, 90(2):127-131.
[16] Nordt, S.P., Clark, R.F.J., 1997. Midazolam: a review of therapeutic uses and toxicity.
J Emerg Med, 15(3):357-365.
[17] Pentikinen, P.J., Vlisalmi, L., Himberg, J.J., 1989. Pharmacokinetics of midazolam following intravenous and oral administration in patients with chronic liver disease and in healthy subjects.
J Clin Pharmacol, 29(3):272-277.
[18] Rosow, C., Manberg, P.J., 2001. Bispectral index monitoring.
Anesthesiol Clin N Amer, 19(4):947-966.
[19] Sandin, M., Thrn, S.E., Dahlqvist, A., 2008. Effects of pain stimulation on bispectral index, heart rate and blood pressure at different minimal alveolar concentration values of sevoflurane.
Acta Anaesthesiol Scand, 52(3):420-426.
[20] Shafer, S.L., Gregg, K.M., 1992. Algorithms to rapidly achieve and maintain stable drug concentrations at the site of drug effect with a computer-controlled infusion pump.
J Pharmacokinet Biopharm, 20(2):147-169.
[21] Smith, C., McEwan, A.I., Jhaveri, R., 1994. The interaction of fentanyl on the Cp50 of propofol for loss of consciousness and skin incision.
Anesthesiology, 81(4):820-828.
[22] Song, J.C., Zhang, M.Z., Lu, Z.J., 2009. The effects of obstructive jaundice on the pharmacodynamics of propofol: does the sensitivity of intravenous anesthetics change among icteric patients?.
Acta Anesthesiol Scand, 53(6):1329-1335.
[23] Song, J.G., Cao, Y.F., Yang, L.Q., 2005. Awakening concentration of desflurane is decreased in patients with obstructive jaundice.
Anesthesiology, 102(3):562-565.
[24] von Moltke, L.L., Greenblatt, D.J., Schmider, J., 1996. Midazolam hydroxylation by human liver microsomes
in vitro: inhibition by fluoxetine, norfluoxetine, and by azole antifungal agents.
J Clin Pharmacol, 36(9):783-791.
[25] White, M., Kenny, G.N., 1990. Intravenous propofol anesthesia using a computerized infusion system.
Anaesthesia, 45(3):204-209.
[26] Wojnowski, L., 2004. Genetics of the variable expression of CYP3A in humans.
Ther Drug Monit, 26(2):192-199.
[27] Wu, J., Huang, S.Q., Chen, Q.L., 2013. The influence of the severity of chronic virus-related liver disease on propofol requirements during propofol-remifentanil anesthesia.
Yonsei Med J, 54(1):231-237.
[28] Yamakura, T., Harris, R.A., 2000. Effects of gaseous anesthetic nitrous oxide and xenon on ligand-gated ion channels. Comparison with isoflurane and ethanol.
Anesthesiology, 93(4):1095-1101.
[29] Yang, L.Q., Song, J.C., Irwin, M.G., 2010. A clinical prospective comparison of anesthetics sensitivity and hemodynamic effect among patients with or without obstructive jaundice.
Acta Anaesthesiol Scand, 54(7):871-877.
[30] Zbinden, A.M., Maggiorini, M., Petersen-Felix, S., 1994. Anesthetic depth defined using multiple noxious stimuli during isoflurane/oxygen anesthesia. I. Motor reactions.
Anesthesiology, 80(2):253-260.

Open peer comments: Debate/Discuss/Question/Opinion
<1>